Studies reveal that breast reduction is associated with the highest satisfaction rate and most profound positive impact on women’s lives. The most frequently expressed sentiment being — Why did I wait so long?
While large breasts are usually inherited, hormones, pregnancy, menopause and weight gain can all contribute to an increase in breast size. Women with excessively large, heavy breasts are good candidates for this surgery. Aside from the psychosocial aspects of large breasts, physical symptoms may include pain in the neck, back and shoulders; rashes in the crease of the breast and poor posture. Lifestyle issues often present themselves as well. Women with very large breasts have trouble finding proper clothing and are unable to participate in activities others take for granted.
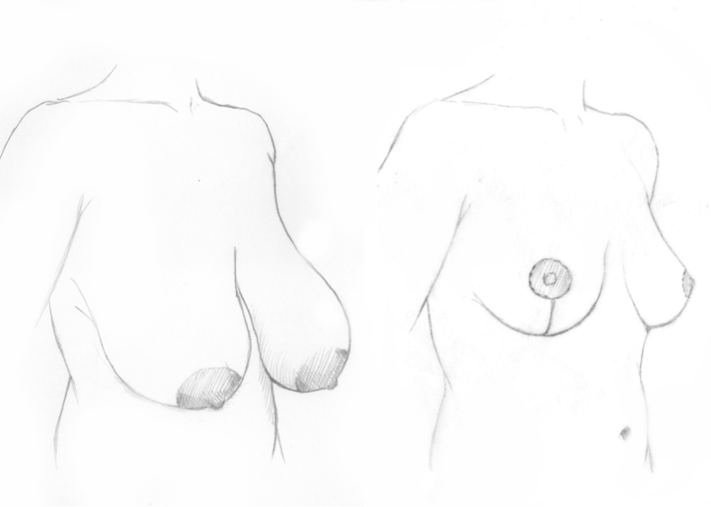
A breast reduction removes excess breast tissue and fat, and sculpts the breast into a smaller, lighter, lifted shape. Incisions are made around the areola, vertically down from the areola to the breast crease and there may be a horizontal scar at the breast crease. Today newer techniques allow for significantly shorter incisions. The type and location of the various incisions are discussed during consultation and are dependent upon your anatomy. Through these incisions, tissue and skin are removed and the nipple is repositioned to match the new breast shape. However, even though the nipple is relocated to a higher position on the breast mound, aside from rare instances, it typically stays attached to the breast tissue, thus maintaining its blood supply.
Priorities
It is important to spend time in consultation understanding desired size and shape. The final size should be proportionate to a woman’s height and overall stature. My priority when performing breast reduction is to create a suitable breast projection and shape, while adjusting the volume, minimizing scars, and retaining nipple sensation. It is crucial to guard the safety of the nipple and areola so that adequate blood flow is insured while tissue is removed. Ideally, the size of the areola should be commensurate with the new size of the breast.
Hirmand Technique
My preferred technique is the more novel “supramedial” pedicle with a short “lollipop” scar. This technique preserves maximum fullness in the top portion of the breasts, maintains robust blood flow to the nipple and areola and allows optimal removal of the extra tissue of the sagging lower part of the breast.
Regardless of the extent of the reduction, this method creates an extraordinary shape and projection with good longevity. Through this approach, the breasts are lifted, made narrower and made more symmetric at the same time. A multilayer closure with absorbable sutures improves scar quality while eliminating the need for suture removal. Sometimes, liposuction of the chest area on the sides of the breast is necessary and can be done effectively at the same time.
A note on liposuction for breast reduction
When can a breast reduction be accomplished using liposuction alone? In a minority of patients whose breasts have a high fat content, no sagging and great skin tone, liposuction alone may deliver the result they seek. The reduction however, is modest.
De-augmentation Reduction, an alternative for some
In a select group of younger women with minimal sagging, good skin tone, and a high glandular content when compared to fat, a “de-augmentation” reduction may be the best procedure if a modest reduction is desired. In this case, no liposuction is performed, nor is it necessary to rearrange the breast tissue. A modest amount of tissue is directly removed through a small incision in the inframammary fold (crease under the breasts) to make the breasts smaller.
Surgical notes
Anesthesia: general
Length of surgery: 4 hours
Outpatient/inpatient: outpatient
Adjunct procedures: liposuction
Recovery: one week